
Six-figure bonuses, closed clinics, and rural care deserts point to a deeper problem: who controls entry into the profession.
High veterinary bills are real. Corporate consolidation is visible. But if corporations caused the veterinary shortage, one fact becomes hard to explain: even the corporations cannot hire enough veterinarians.
Pet owners feel the crisis first as a bill, a wait list, a closed emergency door, or a phone call that ends with “we are not taking new clients.” It is natural to look at clinic roll-ups and assume the shortage must be another story about corporate power. Corporate ownership can make care feel less personal and more expensive. It can reduce local competition. It can change workplace culture. It can create pressure to maximize revenue.
But that is not the same as causing the shortage.
A corporation can buy a clinic. It cannot create veterinary care without veterinarians. If corporate ownership were the source of the shortage, large employers would not need extraordinary signing, retention, relocation, and loan-repayment packages just to get doctors into exam rooms. A profit-seeking employer has no reason to pay more than the market requires. Six-figure recruiting offers are not a sign of abundant labor. They are a distress signal from a market where demand is trying to rise and supply cannot respond fast enough.1
Corporate groups with deep pockets can outbid independent clinics, shelters, nonprofits, and rural practices for the limited pool of veterinarians. That can move veterinarians around. It does not explain why the pool is limited in the first place.
To understand the shortage, follow the levers that control supply. In veterinary medicine, those levers sit upstream from the clinic. They sit in the licensing architecture: who may open a school, who may sit for the national exam, who controls that exam, and whether a veterinarian already trained abroad can enter the workforce here.
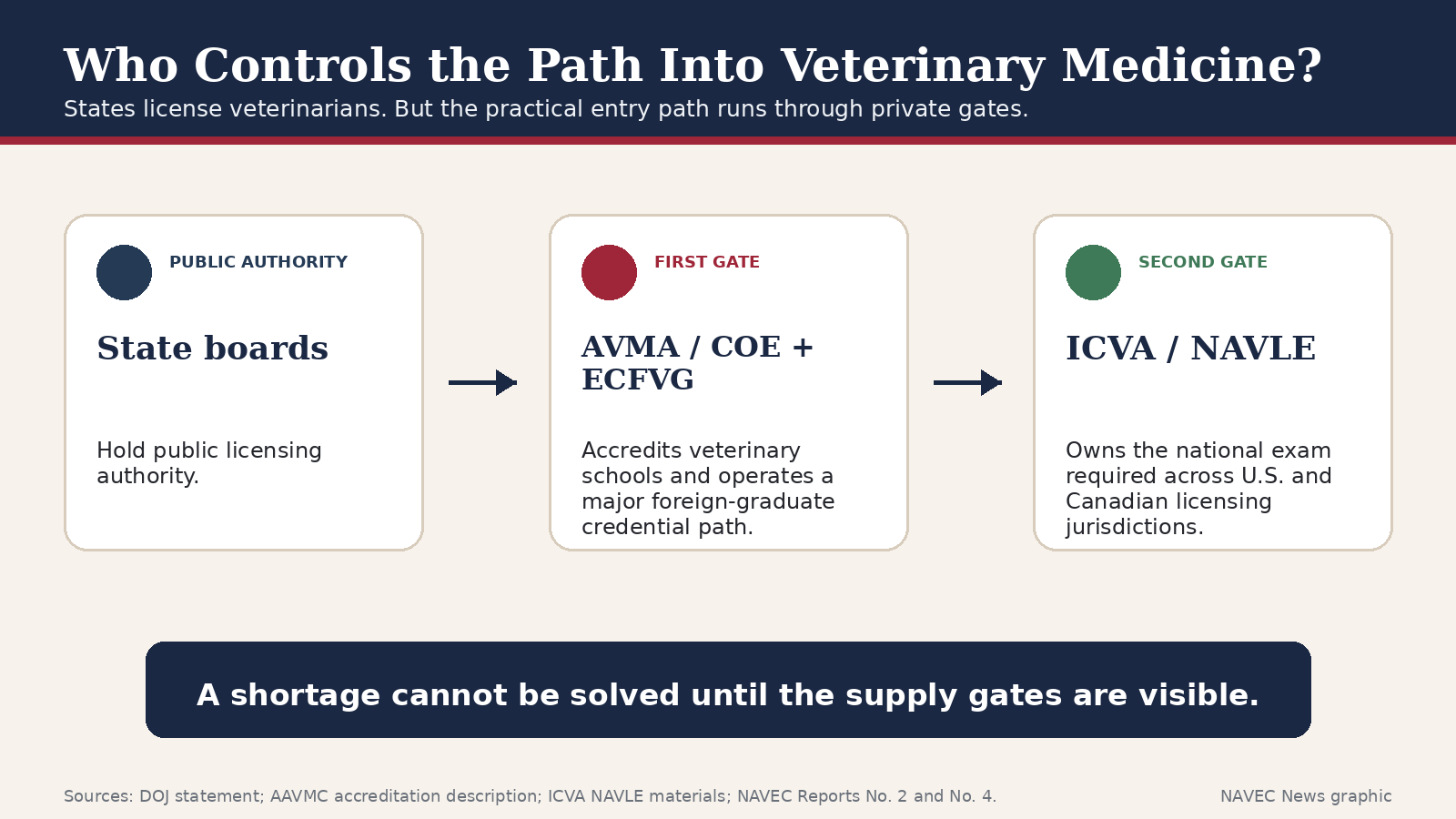
At first glance, veterinary licensure looks like any other professional licensing system. State legislatures write practice acts. State-appointed veterinary boards issue licenses. The public actor is the state board.
The problem is where the state board points the applicant next.
In practice, states have made entry into veterinary medicine depend on private national gatekeepers. A state board may hold the license stamp, but the applicant first must pass through gates the board does not operate, does not audit in any meaningful public way, and often cannot independently verify.
The first gate is the school gate. The AVMA Council on Education is the U.S. Department of Education-approved accrediting agency for veterinary colleges. AAVMC explains that a college must earn COE accreditation to become an AAVMC member institution, and the Justice Department has put the public importance of the gate plainly: for decades, the United States has had only about 34 accredited veterinary colleges, all solely accredited by the AVMA.2
That means AVMA/COE accreditation is not just an academic label. It is the practical condition for opening, expanding, or keeping a veterinary school in the standard U.S. licensure pipeline. Control the accreditation gate and you control, in large part, how many graduates the system can produce.
The AVMA also operates the Educational Commission for Foreign Veterinary Graduates, or ECFVG, a major credential path for internationally trained veterinarians from non-AVMA-accredited schools. A second pathway, AAVSB’s PAVE program, exists and is accepted by many jurisdictions. But the overall foreign-trained route remains narrow, costly, and capacity-limited; the central point is that veterinarians already trained abroad do not enter through a scalable medical-style credential. They enter through a small professional funnel.3
The second gate is the exam gate. ICVA owns and administers the NAVLE, the national exam required for licensure in all U.S. and Canadian licensing jurisdictions. ICVA’s own public materials state that candidates may not review the test after results are released and that rescores or appeals of NAVLE results are not permitted.4
This is the lead: the veterinary shortage is not merely a clinic-level story. It is a licensing architecture story. Public need depends on a supply pipeline controlled through private, profession-controlled chokepoints with limited public supervision, limited transparency, and no real competing gate.
Give a small profession-controlled system every practical key to entry, remove meaningful outside audit, and the risk is predictable: the gate begins to protect the gate.
It is hard to prove motive, and this article does not need to. The stronger case is structural. When the body that controls a supply gate has spent decades warning that the profession has, or soon will have, too many veterinarians, the public should inspect the gate.
That forecast record is not folklore. It is documented in AVMA-commissioned and AVMA-published workforce analyses stretching back nearly fifty years. The recurring institutional warning was surplus, excess capacity, underutilization, stagnant incomes, or caution against expanding supply. To put it mildly, many of those predictions did not age well.
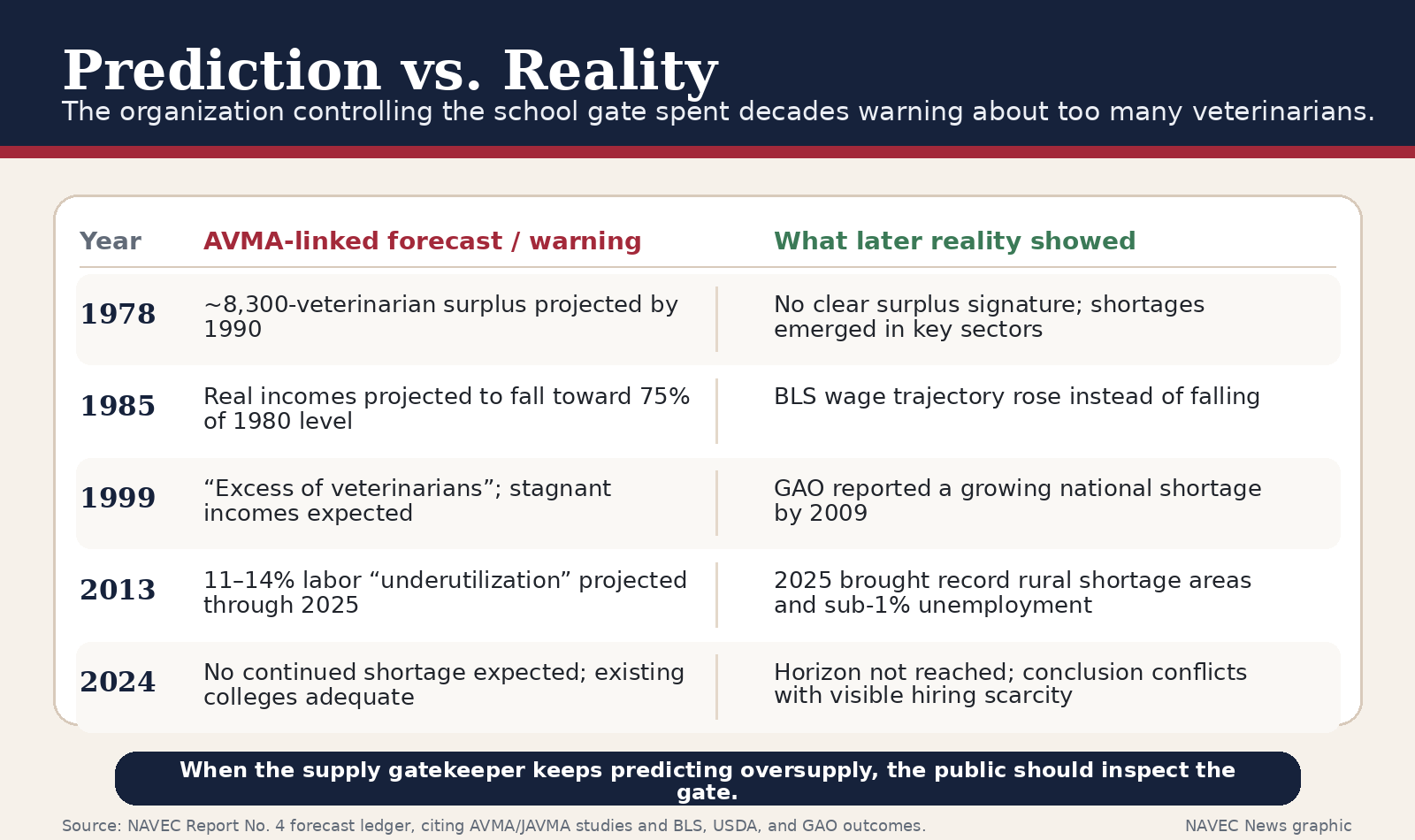
In 1978, the AVMA-commissioned Arthur D. Little study projected a surplus of roughly 8,300 veterinarians by 1990. In 1985, Wise and Kushman projected that private-practitioner real incomes would fall toward 75 percent of their 1980 level by 2000. The 1999 KPMG “Megastudy,” commissioned by AVMA, AAHA, and AAVMC, found evidence of “excess” veterinarians. The 2013 AVMA Workforce Study projected 11–14 percent labor underutilization through 2025. In 2024, an AVMA-commissioned Brakke analysis again concluded that existing colleges were adequate and that the data did not support an expectation of a continued shortage.5
Now compare the prediction record with the world animal owners and employers actually face. The Government Accountability Office warned in 2009 of a growing national shortage. USDA shortage designations have not disappeared; they reached record levels in 2025. BLS projects veterinarian employment growth much faster than average. Veterinarian unemployment fell below one percent. Employers advertise six-figure incentives because they cannot fill jobs. Rural, food-animal, shelter, and public-health roles remain exposed.6
The point is not that every old forecast was foolish. Forecasting is hard. The point is that the same institution repeatedly inclined toward oversupply warnings while also controlling the accreditation lever that determines how many veterinary schools, and therefore how many graduates, may exist. That combination of mindset and power is exactly why public oversight matters.
The NAVLE issue is not simply that candidates dislike a difficult exam. Licensing exams should be difficult. The problem is that this exam is the only national gate, and the public bodies that rely on it have no practical way to verify its fairness from the outside.
NAVEC’s exam investigation describes a narrower, legally important claim: it does not prove that ICVA rigs, biases, or corrupts the NAVLE. It argues that because ICVA controls the exam content, scoring, equating, outcome data, and candidate policies, serious allegations about opacity and discriminatory effect cannot be conclusively proven or credibly disproven by anyone outside ICVA, including the state boards that condition licensure on the exam.7
That should concern every state board. If a state is going to bar a person from a profession, the state should be able to assure the public that the decisive exam is valid, fair, auditable, and merit-based. “Trust the private monopoly” is not an adequate due-process standard for a gate that determines whether a trained veterinarian may work.
The minimum safeguards are not radical: independent psychometric audit, published fairness standards, meaningful appeal rights, de-identified researcher access to outcome data, and public reporting sufficient to show that the exam measures competence rather than rationing entry.
The accreditation side of the gate is no longer a theoretical policy concern. It is now a live antitrust issue.
Lincoln Memorial University sued the AVMA in federal court, alleging that AVMA accreditation practices restrict the number of veterinary schools, the output of veterinary students, and ultimately the number of veterinarians available to the public. Reuters reported that LMU challenges AVMA standards, especially research-related requirements, as unrelated to graduating competent “day-one-ready” veterinarians and as especially burdensome for schools without large endowments or outside funding. The AVMA declined comment to Reuters because of pending litigation.8
The Justice Department then filed a statement of interest in the case. DOJ did not decide LMU’s allegations. But it did state the legal principle that matters to the public: professional accreditation societies, including the AVMA, cannot erect anticompetitive hurdles that reduce competition by restricting the number of providers entering the profession. DOJ also emphasized that accreditors made up of interested market participants face an inherent conflict when regulating entry into a profession, especially when standards are developed behind closed doors.9
That is the accountability opening. A public license cannot be treated as a private club rule when the consequence is fewer veterinarians, longer waits, higher labor costs, rural care deserts, and animals going without care.
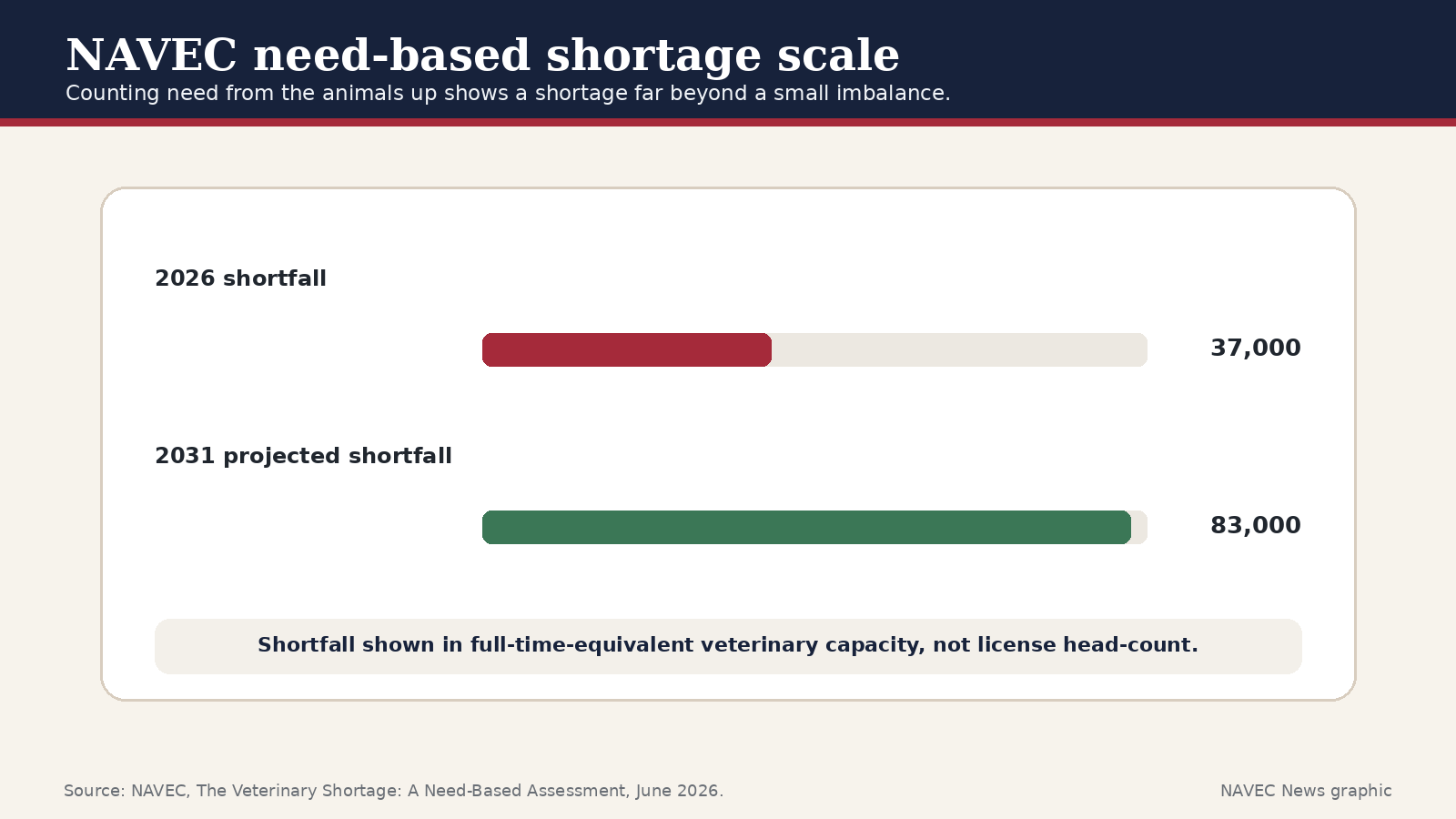
Once the surplus narrative is tested against reality, the next question is measurement. A head count is not enough. A veterinarian can hold a license and work part time, move into relief work, leave clinical practice, work in industry, teach, retire, or serve a metropolitan companion-animal market while rural and shelter systems go uncovered. A license count can look adequate while the exam rooms remain empty.
The logical way to measure the gap is to start from need: the number of animals requiring care, the settings that must be covered, the rural and food-animal infrastructure needed for food security, shelter and nonprofit capacity, public practice, and the full-time equivalent veterinary work actually available to meet that need. Using that need-based approach, the present shortfall is roughly 37,000 full-time veterinarians, widening toward about 83,000 by 2031 if the current structure remains in place.10
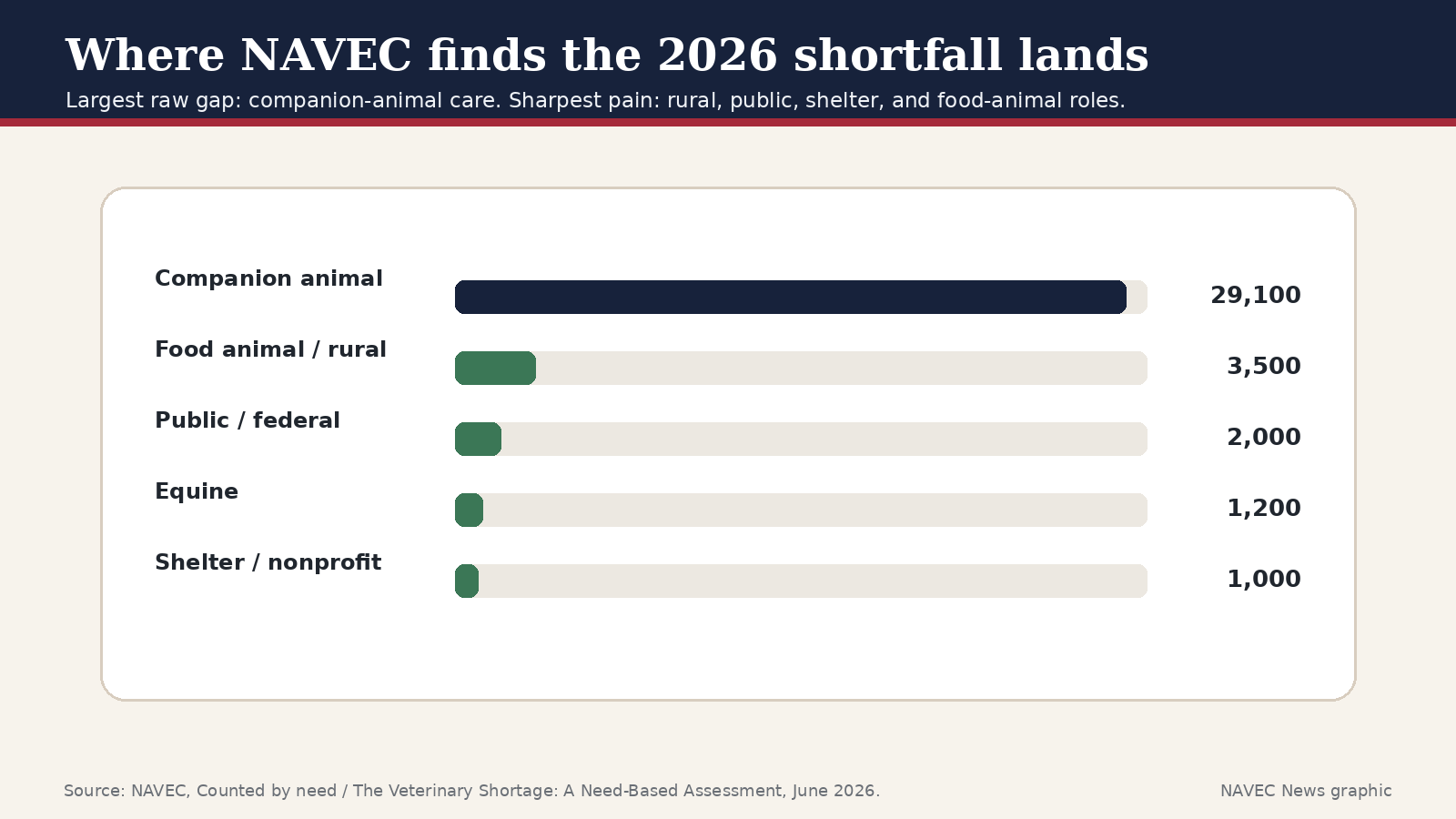
The shortage is not evenly felt. Companion-animal care carries the largest raw number because there are so many pets and visits. But each missing veterinarian can leave an even larger hole in a rural food-animal region, shelter system, equine corridor, or public-health role where there may be no nearby substitute.
The fastest way to relieve a professional shortage is to admit qualified people who are already trained. Veterinary medicine does the opposite. Internationally trained veterinarians face a costly, slow, capacity-limited process. NAVEC’s medical-model analysis describes an ECFVG pathway ending in a three-day hands-on Clinical Proficiency Examination no U.S. graduate takes, offered at only two sites, with roughly 248 new-candidate seats a year and a 2026 CPE fee of $12,804. The result is a trickle: roughly 168 internationally trained veterinarians entering per year.11
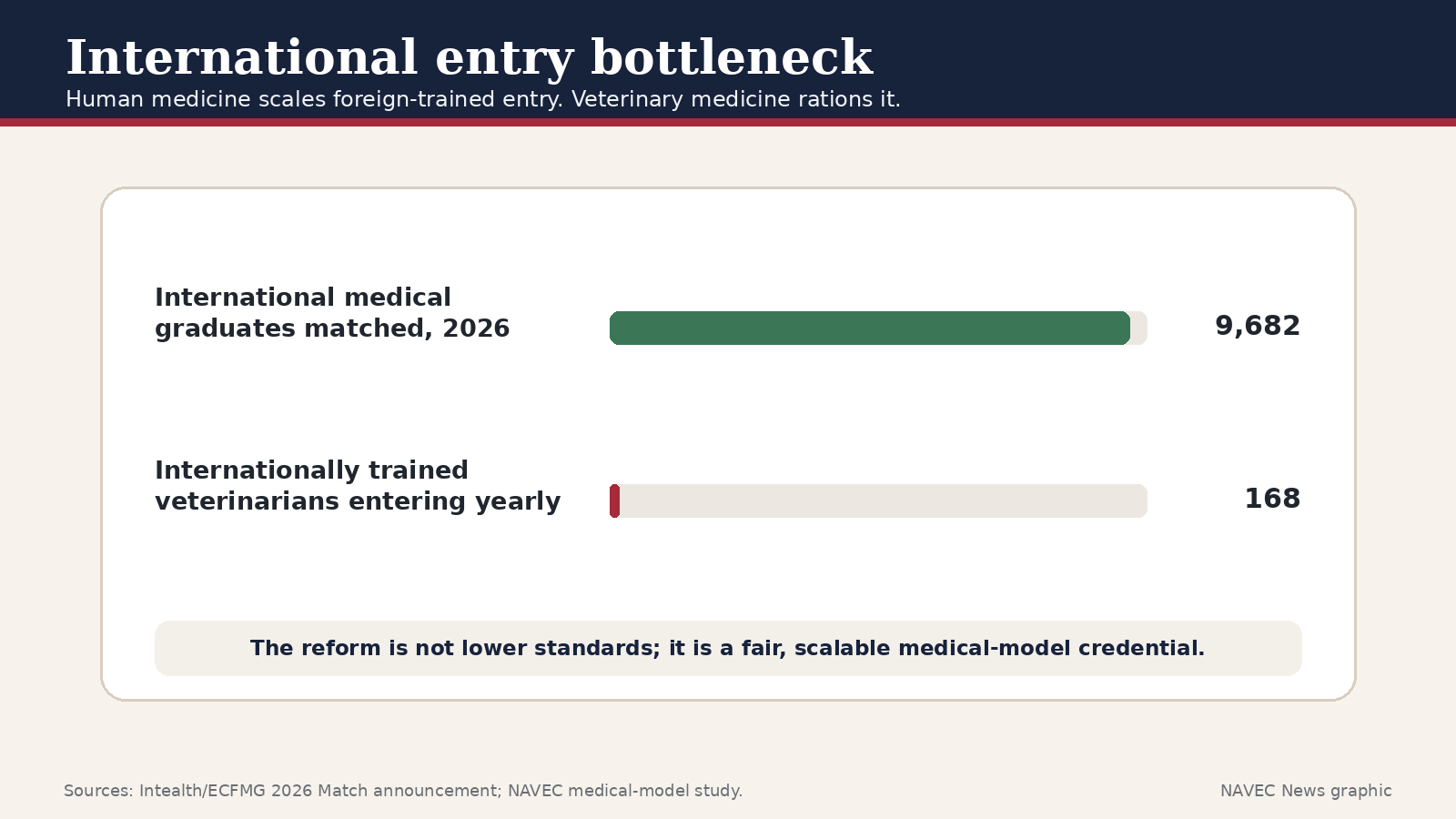
Human medicine made a different choice. In the 2026 Main Residency Match, international medical graduates matched to 9,682 first-year residency positions. Medicine uses standardized credentialing, verified education, knowledge examinations, residency, and supervised practice rather than a tiny practical-exam funnel. Medicine also discontinued USMLE Step 2 Clinical Skills in 2021 rather than rebuilding a capacity-limited clinical-skills chokepoint.12
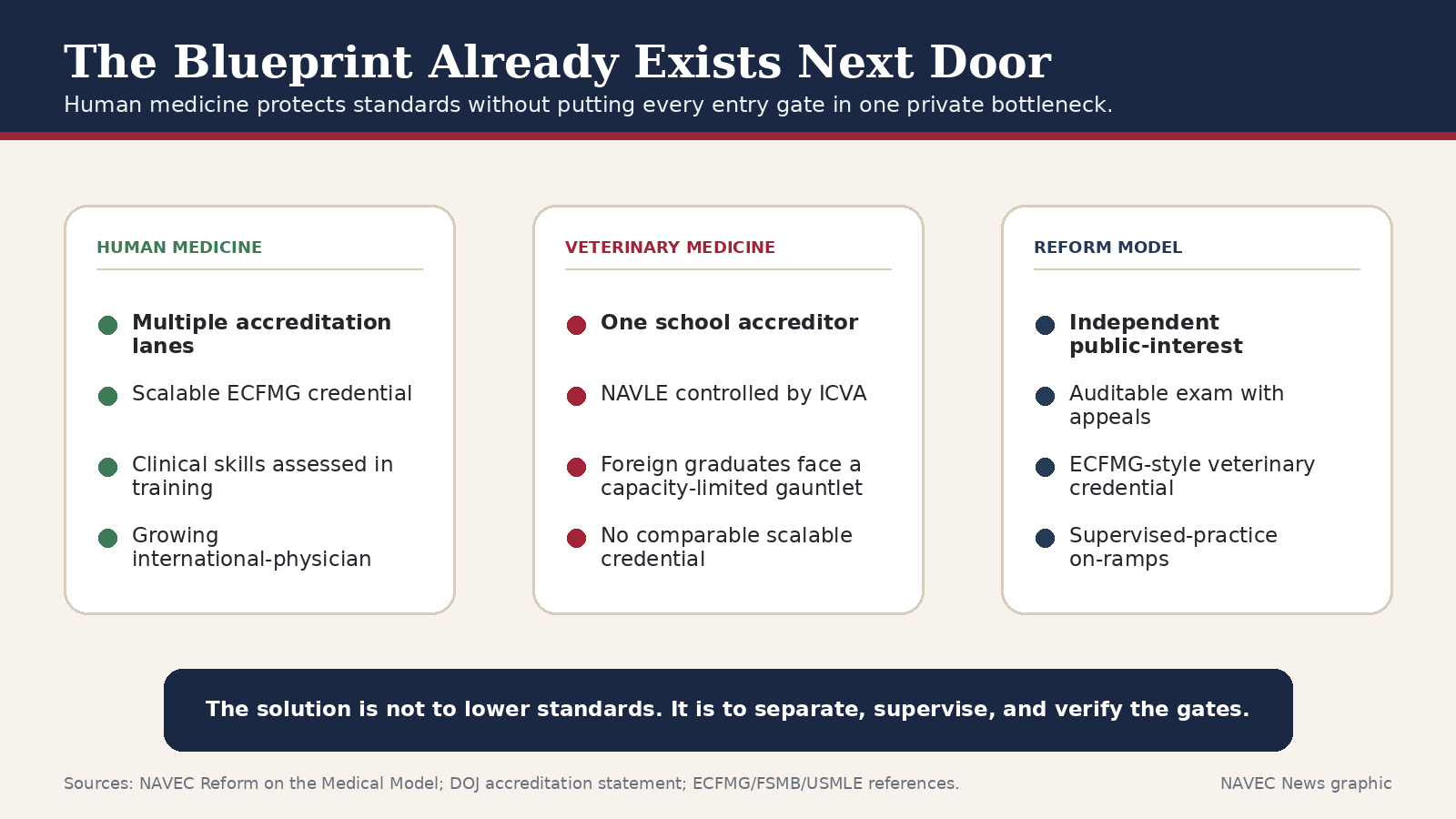
That is the medical model: verify education, test knowledge fairly, supervise practice where needed, publish standards, and let throughput scale. Veterinary medicine could adopt the same logic without lowering standards.
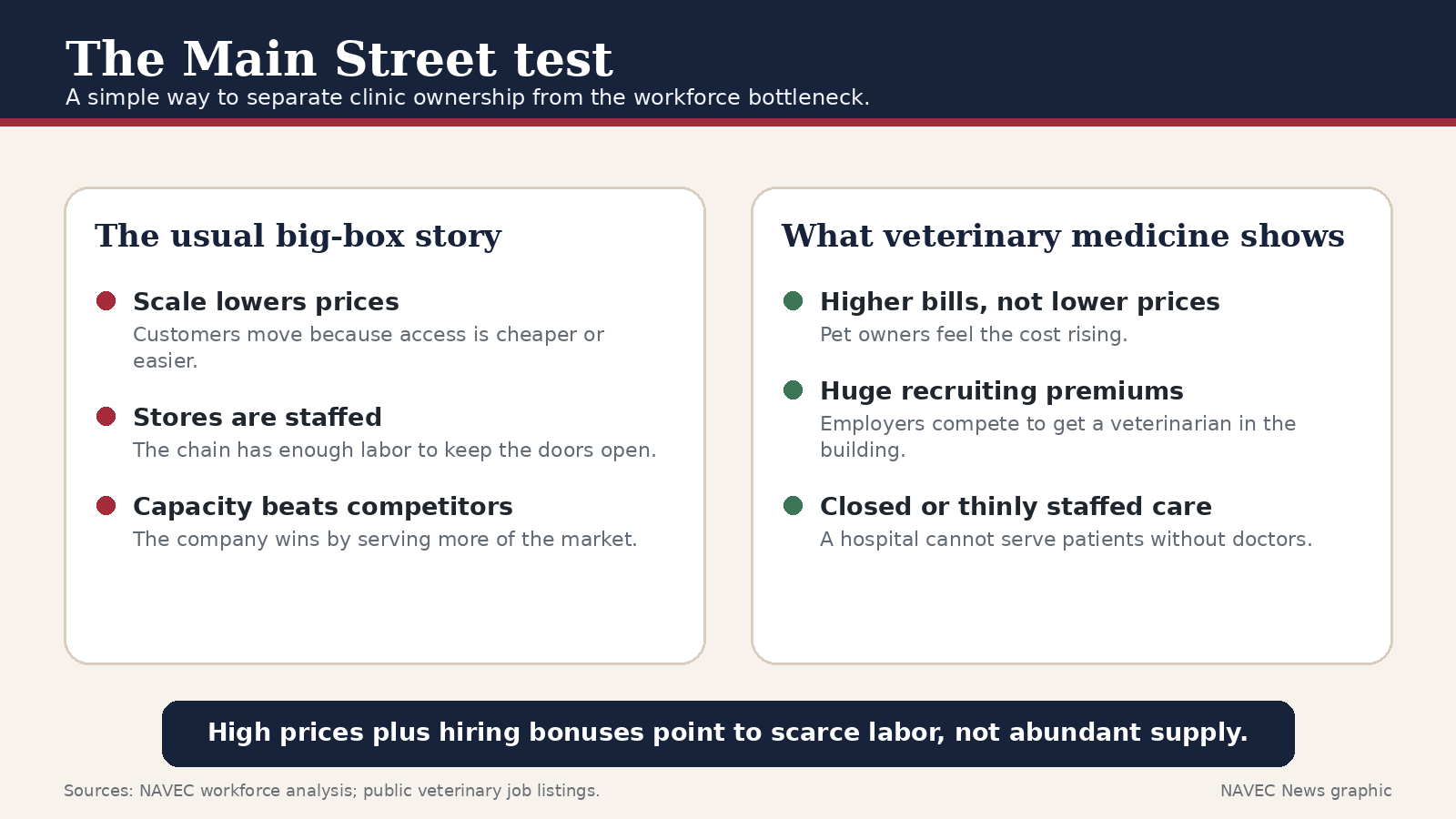
This is why the common corporate explanation feels right but fails as a full diagnosis.
In the familiar big-box story, a giant retailer drives out Main Street by using scale to lower prices competitors cannot match. Veterinary medicine does not fit that pattern. The public is seeing higher bills, not lower ones. Employers are paying more for labor, not less. Some hospitals remain understaffed despite aggressive recruiting. Rural areas often have no corporation to blame because there is no veterinarian at all.
Corporate groups can compete inside the shortage. They can outbid smaller clinics for a scarce doctor. They can move veterinarians from one clinic type to another. But they do not explain why the profession cannot train, test, and admit enough veterinarians to let supply meet need. In a healthy market, rising demand draws new supply. In this market, the demand signal hits a private gate.
The federal process has already begun. The Justice Department has told a federal court that veterinary accreditation standards and procedures are subject to antitrust scrutiny. The next step is state-level scrutiny, because state laws and state boards make the private gates decisive.
State attorneys general should examine whether delegation of practical entry power to AVMA/COE, ECFVG, and ICVA is compatible with antitrust law, due process, and the public interest. State veterinary boards should ask whether they can independently verify the exams and credentials they rely on. Legislators should ask why a public license depends so heavily on private monopoly chokepoints with so little public supervision.
The remedy is not to let unqualified people practice. The remedy is to make the gates lawful, independent, supervised, transparent, and verifiable.
That means: separate school accreditation from trade-association control; create competitive or independent public-interest accreditation pathways; audit the NAVLE and require meaningful appeals; publish fairness and psychometric data; replace the foreign-trained gauntlet with a medical-model credential; and make state boards active supervisors rather than passive recipients of private decisions.
NAVEC exists because the veterinary shortage is not merely a workforce inconvenience. It is an animal-welfare, rural-access, food-security, public-health, and consumer-protection problem. For too long, the most important question was treated as too technical for the public to ask: who controls entry into the profession?
Once that question is visible, the solution becomes easier to see. The public does not need to choose between high standards and access to care. Human medicine shows that a profession can protect standards while opening scalable, auditable, supervised pathways into practice.
The country cannot solve a veterinarian shortage by arguing only about who owns the clinic while ignoring who controls the path into the profession.
Open the school gate. Audit the exam gate. Replace the foreign-trained bottleneck with the medical model. Let supply respond to need.
Examples of current recruiting pressure include public veterinary job postings and student-recruiting materials advertising substantial signing, retention, relocation, and loan-repayment incentives, including Heartland listings advertising up to $100,000 in sign-on bonuses and VCA early-career loan-repayment offers. Heartland job listing; VCA student careers.↩
AAVMC, “Accreditation,” describing COE as the U.S. Department of Education-approved accrediting agency for veterinary colleges and explaining COE accreditation as a condition of AAVMC institutional membership; U.S. Department of Justice statement noting that for decades the United States has had about 34 accredited veterinary colleges, all solely accredited by AVMA. AAVMC Accreditation; DOJ statement.↩
AVMA, Educational Commission for Foreign Veterinary Graduates / ECFVG materials; AAVSB, PAVE international pathway materials and jurisdiction acceptance information. AVMA ECFVG; AAVSB PAVE; PAVE jurisdiction acceptance.↩
ICVA, “NAVLE,” and NAVLE candidate materials stating that the NAVLE is required for licensure across U.S. and Canadian licensing jurisdictions and that candidates may not review the test after score release; rescores or appeals of NAVLE results are not permitted. ICVA NAVLE.↩
NAVEC Report No. 4, “The Gatekeepers and the Gate,” forecast ledger compiling AVMA-commissioned and AVMA-published workforce analyses from 1978 through 2024, including Arthur D. Little, Wise and Kushman, KPMG, the 2013 AVMA Workforce Study, the 2015 capacity reports, and the 2024 Brakke/Volk analysis. Download Report No. 4.↩
Independent reality checks include GAO-09-178, Bureau of Labor Statistics veterinarian outlook and wage data, USDA/NIFA shortage designations, and the shortage record summarized in NAVEC Report No. 4. GAO report; BLS Occupational Outlook Handbook; NAVEC Report No. 4.↩
NAVEC Report No. 2, “The Gatekeeper No One Can Audit,” and ICVA NAVLE public materials. The report treats allegations as serious and structurally unverified, not as proven findings of misconduct. Download Report No. 2; ICVA NAVLE.↩
Reuters, “US veterinary association sued over alleged antitrust scheme,” June 20, 2025; Lincoln Memorial University complaint and public statement. Reuters reports that AVMA declined comment because of pending litigation. Reuters; LMU public statement.↩
U.S. Department of Justice, “Justice Department Reaffirms Veterinary Accreditation Standards and Procedures Are Subject to Antitrust Scrutiny,” Dec. 15, 2025. DOJ statement.↩
NAVEC Report No. 1, “The Veterinary Shortage: A Need-Based Assessment,” and NAVEC Newsroom, “Counted by need, America is short 37,000 veterinarians — and climbing.” Download Report No. 1; Counted by need.↩
NAVEC, “Reform on the Medical Model,” summarizing the ECFVG bottleneck, CPE cost and seat limits, and foreign-trained veterinarian throughput. Download Reform on the Medical Model.↩
ECFMG / Intealth report on 9,682 international medical graduates matching to first-year residency positions in the 2026 Main Residency Match; USMLE announcement discontinuing work to relaunch Step 2 Clinical Skills. ECFMG / Intealth; USMLE.↩